
Newsom, wife & doctors’ lobby executives attending wine country dinner party
Newsom, wife & doctors’ lobby executives attending wine country dinner party
https://youtu.be/uEo3rnU12jw
Posted November 17, 2020
[UPDATE: Youtube has removed audio. Transcript is provided below.]
The audio (above) is an Edmonton City Council Community and Public Services Committee meeting privately recorded in Alberta, Canada last week.
Dr. Roger Hodkinson is the former Chairman of the Royal College of Physicians and Surgeons committee in Ottawa, he was once CEO of a large private medical laboratory in Edmonton, Alberta, and for the past 20 years has held the position as Chairman of a Medical Biotechnology company based in North Carolina currently tasked with selling a COVID-19 test. He is a medical specialist in pathology, which includes virology, who trained at Cambridge University in the UK — he is perfectly positioned to speak on this topic.
Thank you very much. I do appreciate the opportunity to address you on this very important matter. What I’m going to say is lay language, and blunt. It is counter-narrative, and so you don’t immediately think I’m a quack, I’m going to briefly outline my credentials so that you can understand where I’m coming from in terms of knowledge base in all of this.
I’m a medical specialist in pathology which includes virology. I trained at Cambridge University in the UK. I’m the ex-president of the pathology section of the Medical Association. I was previously an assistant professor in the Faculty of Medicine doing a lot of teaching. I was the chairman of the Royal College of Physicians of Canada Examination Committee and Pathology in Ottawa, but more to the point I’m currently the chairman of a biotechnology company in North Carolina selling the COVID-19 test.
And [inaudible] you might say I know a little bit about all of this. The bottom line is simply this: There is utterly unfounded public hysteria driven by the media and politicians. It’s outrageous. This is the greatest hoax ever perpetrated on an unsuspecting public. There is absolutely nothing that can be done to contain this virus. Other than protecting older, more vulnerable people. It should be thought of as nothing more than a bad flu season. This is not Ebola. It’s not SARS. It’s politics playing medicine and that’s a very dangerous game.
There is no action of any kind needed other than what happened last year when we felt unwell. We stayed home, we took chicken noodle soup, we didn’t visit granny and we decided when we would return to work. We didn’t need anyone to tell us.
Masks are utterly useless. There is no evidence base for their effectiveness whatsoever. Paper masks and fabric masks are simply virtue-signaling. They’re not even worn effectively most of the time. It’s utterly ridiculous. Seeing these unfortunate, uneducated people — I’m not saying that in a pejorative sense — seeing these people walking around like lemmings, obeying without any knowledge base, to put the mask on their face.
Social distancing is also useless because COVID is spread by aerosols which travel 30 meters or so before landing. Enclosures have had such terrible unintended consequences. Everywhere should be opened tomorrow as well as was stated in the *Great Barrington Declaration that I circulated prior to this meeting.
And a word on testing: I do want to emphasize that I’m in the business of testing for COVID. I do want to emphasize that positive test results do not, underlined in neon, mean a clinical infection. It’s simply driving public hysteria and all testing should stop. Unless you’re presenting to the hospital with some respiratory problem.
All that should be done is to protect the vulnerable and to give them all in the nursing homes that are under your control, give them all 3,000 to 5,000 international units of vitamin D every day which has been shown to radically reduce the likelihood of Infection.
And I would remind you all that using the province’s own statistics, the risk of death under 65 in this province is one in 300,000. One in 300,000. You’ve got to get a grip on this.
The scale of the response that you are undertaking with no evidence for it is utterly ridiculous given the consequences of acting in a way that you’re proposing. All kinds of suicides, business closures, funerals, weddings etc. It’s simply outrageous! It’s just another bad flu and you’ve got to get your minds around that.
Let people make their own decisions. You should be totally out of the business of medicine. You’re being led down the garden path by the chief medical officer of health for this province. I am absolutely outraged that this has reached this level. It should all stop tomorrow.
Thank you very much.
.
CASES PER DAY:
DEATHS PER DAY: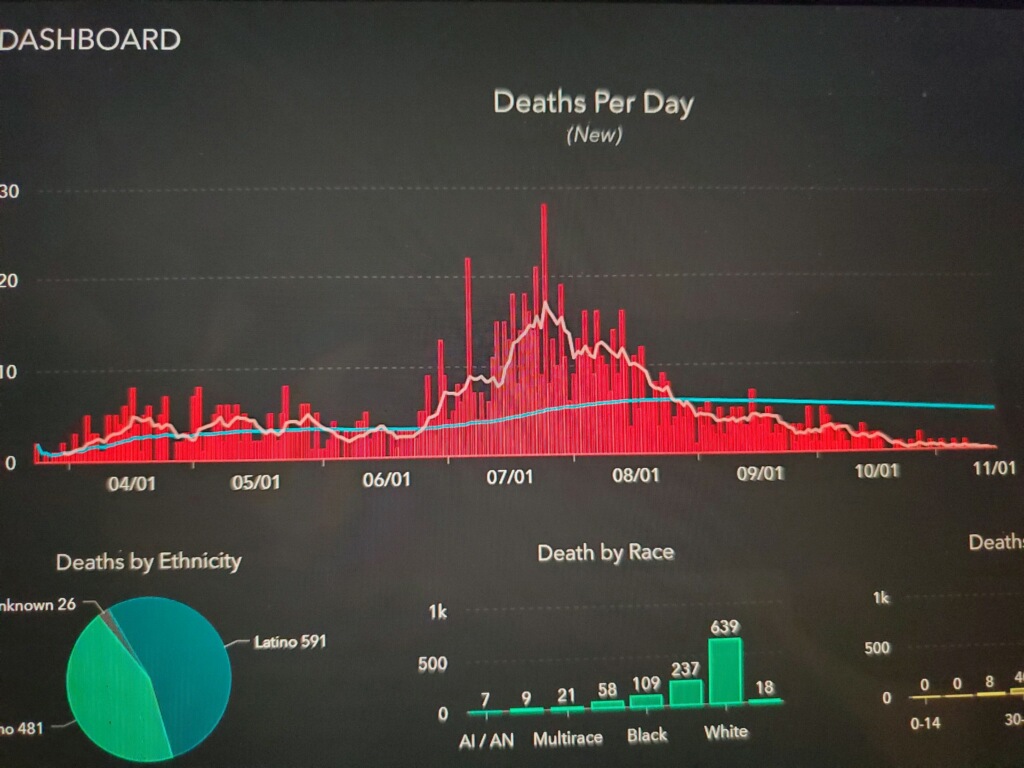
Professor Doctor Sucharit Bhakdi, author of CORONA, FALSE ALARM? Facts & Figures sits down for interview:
https://youtu.be/ZnpnBYgGARE
In this interview Dr. Sucharit references The Great Barrington Declaration.
Manchester University students herded like cattle behind fences over Corona threat.
Hospital bed utilization:
Average 2016-18 -VS- 2020 (for Nov 1-9)
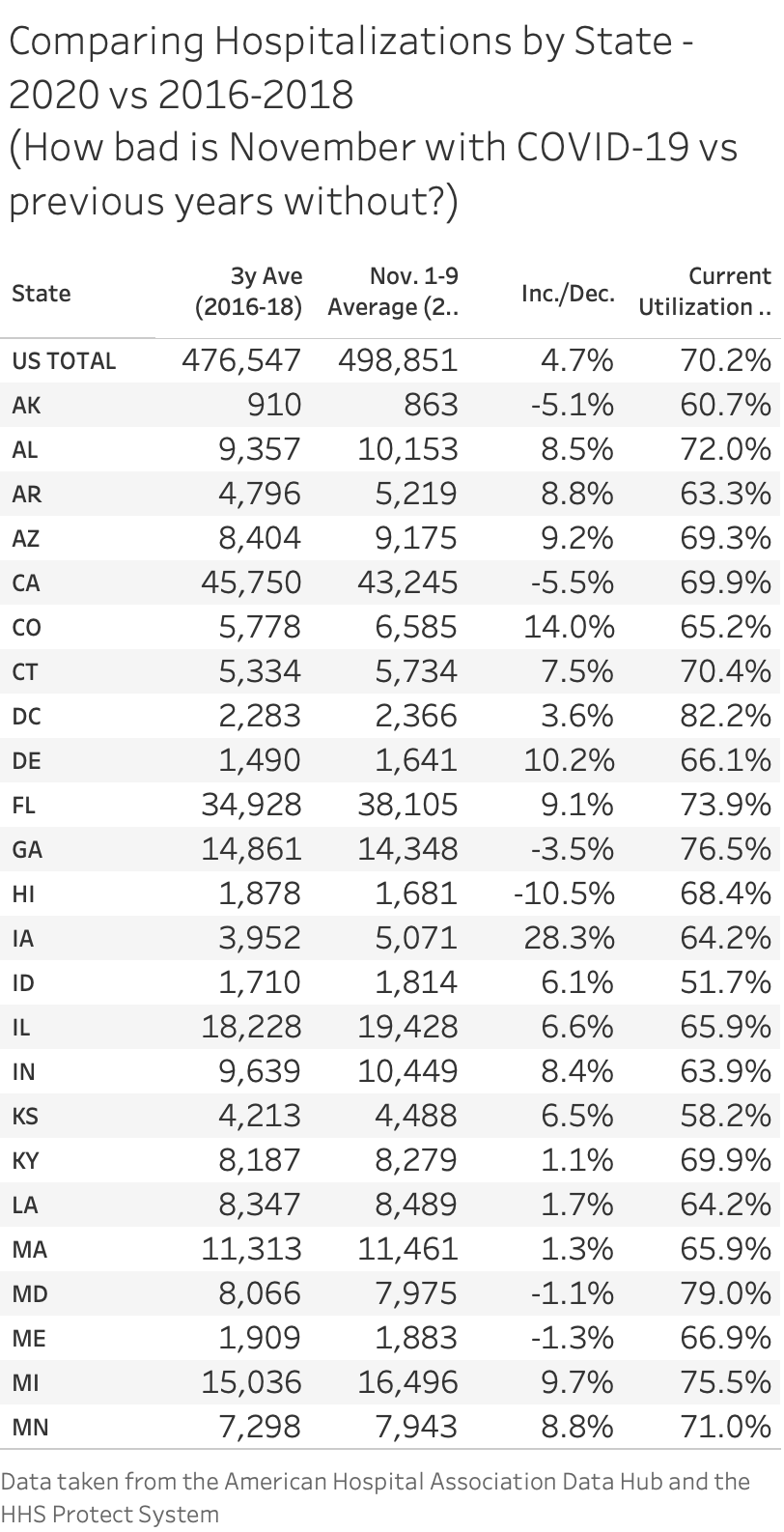
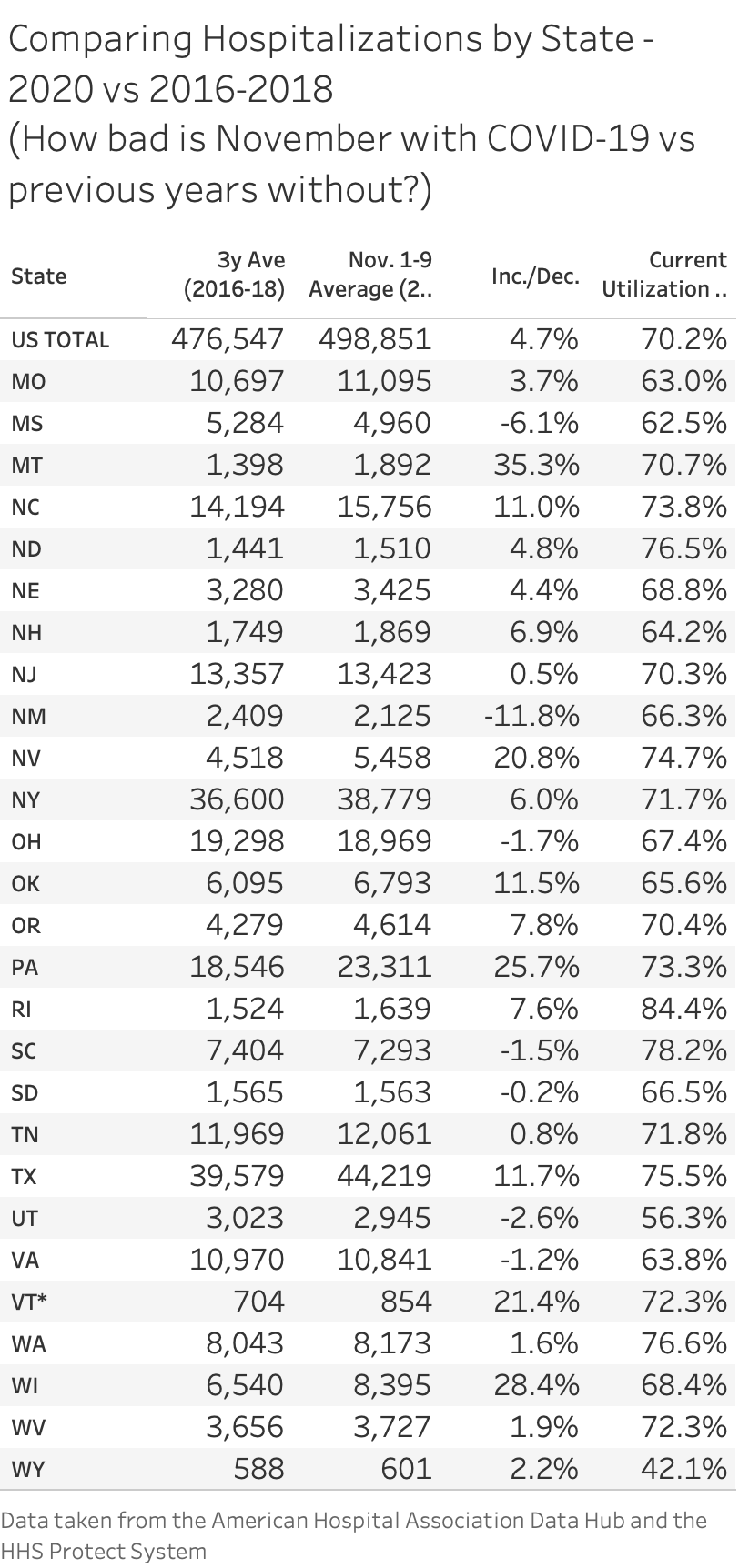
Important to read questions/comments below tables in following post.
https://mobile.twitter.com/justin_hart/status/1327740997078380544
All data taken from:
1) The AHA data hub: guide.prod.iam.aha.org/stats/states
2) The HHS Protect Datasets:
protect-public.hhs.gov
After experiencing cold symptoms Elon Musk was tested four times with mixed results:
Something extremely bogus is going on. Was tested for covid four times today. Two tests came back negative, two came back positive. Same machine, same test, same nurse. Rapid antigen test from BD.
– Elon Musk
Nov 12, 2020
Video published Nov 10, 2020
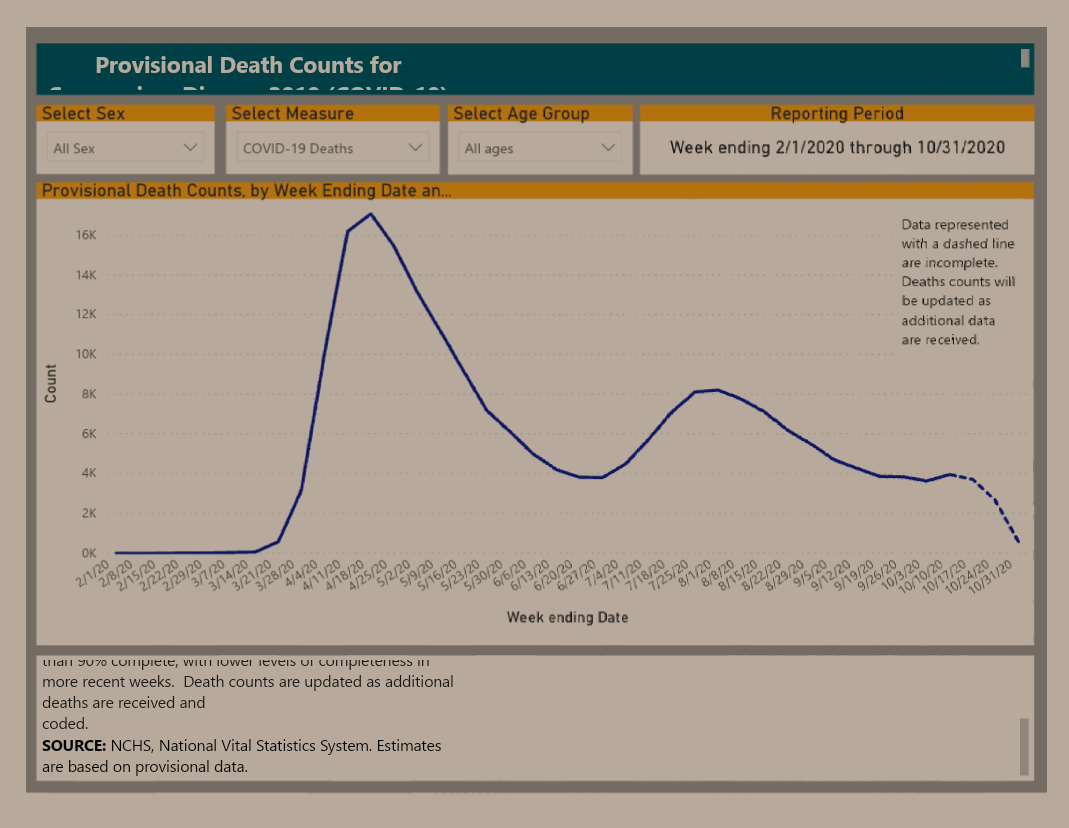 Source: CDC
Source: CDC
“
Provisional death counts deliver the most comprehensive picture of lives lost to COVID-19. These estimates are based on
incoming death certificates, which are the most reliable source of death data and contain information not available anywhere
else, including information about the place of death, other causes that contributed to the death, and race and ethnicity. – CDC
https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm#AgeAndSex